
Source: Lew Rockwell | VIEW ORIGINAL POST ==>
The more I study science, and particularly medicine, the more I come to see how often fundamental facts end up being changed so that a profitable industry can be created. Recently I showed how this happened with blood pressure, as rather than causing arterial damage, high blood pressure is a response to arterial damage that ensures damaged arteries can still bring blood to the tissues and, in turn, rather than helping patients, aggressively lowering blood pressure can be quite harmful. In this article, I will look at the other half of the coin, the Great Cholesterol Scam—something that harms so many Americans it was recently discussed by Comedian Jimmy Dore.
Note: a link to the Dore’s segment can be found here.
Cholesterol and Heart Disease
Frequently, when an industry harms many people, it will create a scapegoat to get out of trouble. Once this happens, a variety of other sectors will jump on the bandwagon and create an unshakable societal dogma. For example, the health of a population (or if they are being poisoned by environmental toxins) determines how easily an infectious disease can sweep through a population and who is susceptible to it, but reframing infectious diseases as a “deficiency of vaccines” it both takes the (costly) onus off the industries to clean up the society and simultaneously allows them to get rich promoting the pharmaceutical products that “manage” each epidemic and the even larger epidemic of chronic diseases caused by those vaccines (discussed in detail here).
Note: the major decline in infectious illness that is credited to vaccines actually was a result of improved public sanitation, and when the data is examined (e.g., for smallpox) those early vaccination campaigns made things worse not better.
In the 1960s and 1970s, a debate emerged over what caused heart disease. On one side, John Yudkin effectively argued that the sugar being added to our food by the processed food industry was the chief culprit. On the other side, Ancel Keys (who attacked Yudkin’s work) argued that it was due to saturated fat and cholesterol.
Note: leaders in the field of natural medicine, like Dr. Mercola, have made a strong case this spike came from the mass adoption of seed oils (which thanks to our unprecedented political climate is at last being discussed on the mainstream news&). Likewise, some believe the advent of water chlorination was responsible for this increase.
Ancel Keys won, Yudkin’s work was largely dismissed, and Keys became nutritional dogma. A large part of Key’s victory was based on his study of seven countries (Italy, Greece, Former Yugoslavia, Netherlands, Finland, America, and Japan), which showed that as saturated fat consumption increased, heart disease increased in a linear fashion.
However, what many don’t know (as this study is still frequently cited) is that this result was simply a product of the countries Keys chose (e.g., if Finland, Israel, Netherlands, Germany, Switzerland, France, and Sweden had been chosen, the opposite would have been found).
Fortunately, it’s gradually become recognized that Keys did not accurately report his data For example, recently an unpublished 56 month randomized study of 9,423 adults living in state mental hospitals or a nursing home (which made it possible to rigidly control their diets) was unearthed. . This study, which Keys was the lead investigator of, found that replacing half of one’s animal (saturated) fats with seed oil (e.g., corn oil) lowered their cholesterol, but for every 30 points it dropped, their risk of death increased by 22 percent (which roughly translates to each 1% drop in cholesterol raising the risk of death by 1%).
Note: the author who unearthed that study also discovered another (unpublished) study from the 1970s of 458 Australians, which found that replacing some of their saturated fat with seed oils increased their risk of dying by 17.6%
Likewise, recently, one of the most prestigious medical journals in the world published internal sugar industry documents. They showed the sugar industry had used bribes to make scientists place the blame for heart disease on fat so Yudkin’s work would not threaten the sugar industry. In turn, it is now generally accepted that Yudkin was right, but nonetheless, our medical guidelines are still largely based on Key’s work.
However, despite a significant amount of data that now shows lowering cholesterol is not associated with a reduction in heart disease, (e.g., this study, this study, this study, this review, this review, and this review) the need to lower cholesterol is still a dogma within cardiology. For example, how many of you have heard of this 1986 study which was published in the Lancet which concluded:
During 10 years of follow-up from Dec 1, 1986, to Oct 1, 1996, a total of 642 participants died. Each 1 mmol/L increase in total cholesterol corresponded to a 15% decrease in mortality (risk ratio 0–85 [95% Cl 0·79–0·91]).
Statins Marketing
One of the consistent patterns I’ve observed within medicine is that once a drug is identified that can “beneficially” change a number, medical practice guidelines will gradually shift to prioritizing treating that number and before long, rationals will be created that require more and more of the population to be subject to that regimen. Consider for example the history of the (immensely harmful) blood pressure guidelines:
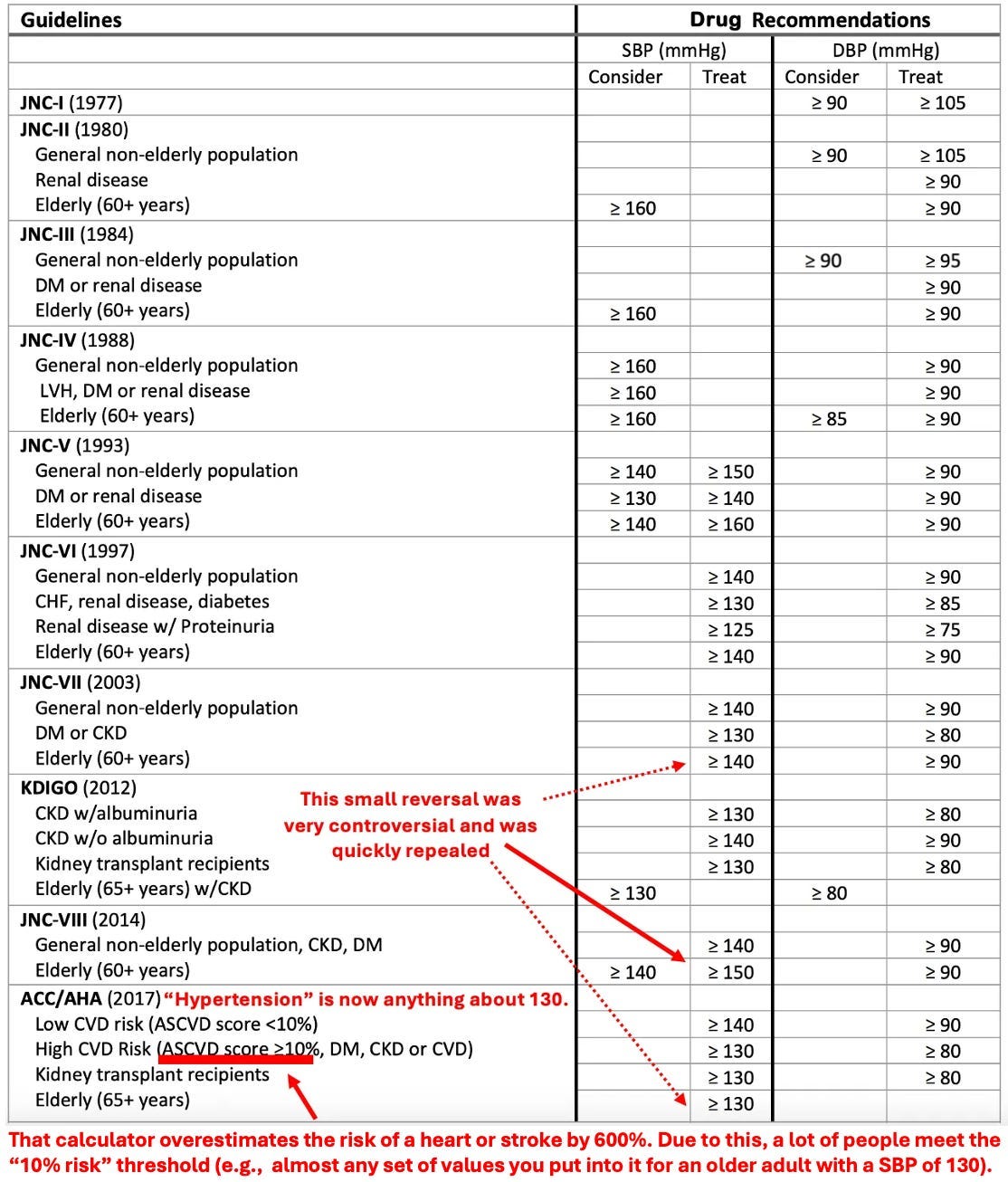
click to enlarge
In the case of statins, prior to their discovery, it was difficult to reliably lower cholesterol, but once they hit the market, research rapidly emerged arguing for a greater and greater need to lower cholesterol, which in turn led to more and more people being placed on statins.

As you would expect, similar increases also occurred within the USA. For example, in 2008-2009, 12% of Americans over 40 reported taking a statin, whereas in 2018-2019, that had increased to 35% of Americans.
Given how much these drugs are used, it then raises a simple question—how much benefit do they produce?
As it turns out, this is a remarkably difficult question to answer as the published studies use a variety of confusing metrics to obfuscate their data (which means that the published statin trials almost certainly inflate the benefits of statin therapy), and more importantly, virtually all of the data on statin therapy is kept by a “private” (industry-funded) research collaboration that consistently publishes glowing reviews of statins (and attacks anyone who claims otherwise) but simultaneously refuses to release their data to outside researchers, which has led to those researchers attempting to get this missing data from the drug regulators.
Note: as discussed in Dr. Malhotra’s interview below, this collaboration (which militantly insists less than 1% of statin users experience side effects) also created a test one could utilize to determine if one was genetically at risk for a statin injury—and in their marketing for the test said 29% of all statin users were likely to experience side effects (which they then removed once health activists publicized this hypocrisy).
Nonetheless, when independent researchers looked at the published trials (which almost certainly inflated the benefit of statin therapy) they found that taking a statin daily for approximately 5 years resulted in you living, on average, 3-4 days longer. Sadder still, large trials have found this minuscule “benefit” is only seen in men. In short, most of the benefit from statins is from creative ways to rearrange data and causes of death, not any actual benefit.
Note: this is very similar to Pfizer’s COVID vaccine trial which professed to be “95% effective” against COVID-19, but in reality only created a 0.8% reduction in minor symptoms of COVID (e.g., a sore throat) and a 0.037% reduction in severe symptoms of COVID (with “severe” never being defined by Pfizer). This in turn meant that you needed to vaccinate 119 people to prevent a minor (inconsequential) case of COVID-19, and 2711 to prevent a “severe” case of COVID-19. Worse still, a whistleblowers later revealed that these figures were greatly inflated as individuals in the (unblinded) vaccine group who developed COVID-19 like symptoms weren’t tested for COVID-19 and their vaccine injuries were never reported. Sadly, in most cases (e.g., the statin trials) we don’t have access to whistleblowers who can inform us of how unsafe and ineffective these drugs actually are.
In circumstances like these where an unsafe and ineffective but highly lucrative drug must be sold, the next step is typically to pay everyone off to promote it. For example: to quote Chapter 7 of Doctoring Data:
The National Cholesterol Education Programme (NCEP) has been tasked by the National Institutes of Health to develop guidelines [everyone uses] for treating cholesterol levels. Excluding the chair (who was by law prohibited from having financial conflicts of interest), the other 8 members on average were on the payroll of 6 statin manufacturers.
In 2004, NCEP reviewed 5 large statin trials and recommended: “Aggressive LDL lowering for high-risk patients [primary prevention] with lifestyle changes and statins.”
In 2005 a Canadian division of the Cochrane Collaboration [who were not paid off] reviewed 5 large statin trials (3 were the same as NCEP’s, while the other 2 had also reached a positive conclusion for statin therapy). That independent assessment instead concluded: “Statins have not been shown to provide an overall health benefit in primary prevention trials.”
Note: the primary reason no cure for COVID-19 was ever found was that the guideline panel for COVID-19 treatments was handpicked by Fauci and comprised of academics taking money from Remdesivir’s manufacturers. Not surprisingly, the panel always voted against recommending any of the non-patentable treatments for COVID-19, regardless of how much evidence there was for them.
Likewise, the American College of Cardiology made a calculator to determine your risk of developing a heart attack or stroke in the next ten years based on your age, blood pressure, cholesterol level, and smoking status. In turn, I’ve lost track of how many doctors I saw proudly punch their patient’s numbers into it and then inform them that they were at high risk of a stroke or heart attack and urgently needed to start a statin. Given that almost everyone ended up being “high risk” I was not surprised to learn that in 2016, Kaiser completed an extensive study which determined that this calculator overestimated the rate of these events by 600%. Sadly, that has not at all deterred the use of this calculator (e.g., medical students are still tested on it for their board examinations).
Note: one of the most unfair things about statins is that the healthcare system decided they are “essential” for your health, so doctors who don’t push them are financially penalized, and likewise patients who don’t take them are as well (e.g., through life insurance premiums).
So, despite the overwhelming evidence against their use, many physicians believe so deeply in the “profound” benefits of statins that they do things like periodically advocating for statins to be added to the drinking water supply.